SYNCOPE ASSESSMENT AND TILT TESTING
It is not just a simple faint
WHAT IS SYNCOPE?
Syncope is defined as transient loss of consciousness (TLOC) due to cerebral hypoperfusion. [1]
Although characterized by swift onset, short duration, and spontaneous complete recovery [1], “Syncope is an alarming event carrying the possibility of serious outcomes” [2], including potentially life-threatening heart condition and sudden cardiac death (SCD). [2.3]
FACTS & PREVALENCE
50% of the population will faint at least once in their lifetime. [3]

Syncope presents across all age groups
- The median age of the first syncope is approximately 14 years. [4]
- Most people with vasovagal syncope will have had their first syncope before age 40. [4]
- The incidence of syncope in the ED increases with age, with a sharp rise in patients older than 70 years. [5]
Syncope is frequent which causes high financial costs
- 1 in 6 admissions to hospital are due to syncope [3], and Syncope accounts for up to 3% of all emergency department (ED) visits. [5]
- “The financial burden for healthcare systems is substantial as syncope hospitalizations confer an annual cost of $1.7 billion, and up to $26,000 per hospitalization.” [6]
- Many implications and costly test procedures might be saved if the recommendations of the ESC Syncope Guidelines, which include continuous blood pressure measurement in the course of tilt table testing (HUT), are taken into account right after initial assessment. [7]
CHALLENGES
Syncope accounts for up to 3% of all emergency department (ED) visits5, however approximately 35% of patients with syncope remain undiagnosed in the ED. 4
Syncope is a diagnostic challenge with complex underlying mechanisms 2,8, requiring multidimensional approaches and individualized patient management.
DIAGNOSTIC PATH FOR UNEXPLAINED SYNCOPE
(acc. ESC Guidelines)

- In many cases an efficient initial syncope evaluation can lead to diagnosis and start of treatment. [1]
- In cases with uncertain diagnosis and suspected cardiac origin, cardiac evaluation is performed. [1]
- In all other cases with frequent or severe episodes, cardiovascular autonomic function tests are recommended. This makes the majority of the patients. [1]
- Head up Tilt Test (HUT) provides high diagnostic yield and is recommended by the ESC guidelines in case of suspicion of syncope after an initial inconclusive evaluation. [1,7]
CONTINUOUS MEASUREMENTS FOR CARDIOVASCULAR AUTONOMIC FUNCTION TESTS
As the onset of syncope happens extremely fast [1] only continuous measurements are helpful to caputure an event.
- Cardiovascular autonomic function tests require synchronized measurement of ECG (min 3 leads) and blood pressure, both in a continuous manner. [1]
- Beat-to-beat blood pressure monitoring is recommended in several guidelines and expert consenses due to “the context of syncope blood pressure (BP) can change substantially in a few seconds”. [9]
- “Conventional intermittent BP measurements allow one measurement per minute at best and are therefore unsuitable for syncope assessment.” [9]
“Our patients seek solutions, not only explanations.“ [1]
EXPERTS
ON SYNCOPE
“If I had the option to ask the industry for one thing in the future, it would be to have a device that can measure blood pressure at the time of syncope. This is my most important requirement.” [ Prof. Michele Brignole, Italy ]
EASY TO USE INNOVATIVE TOOLS
With more than 20 years experience CNSystems provides you with state-of-the-art devices for high level syncope assessment.
- Continuous blood pressure measurement from the unique CNAP® finger sensor
- Advanced hemodynamic evaluation using CNAP® HD technology ) – non-invasive
- Synchronized patient signals (incl. wireless 12-lead ECG)
- Truly continuous recording when it matters most
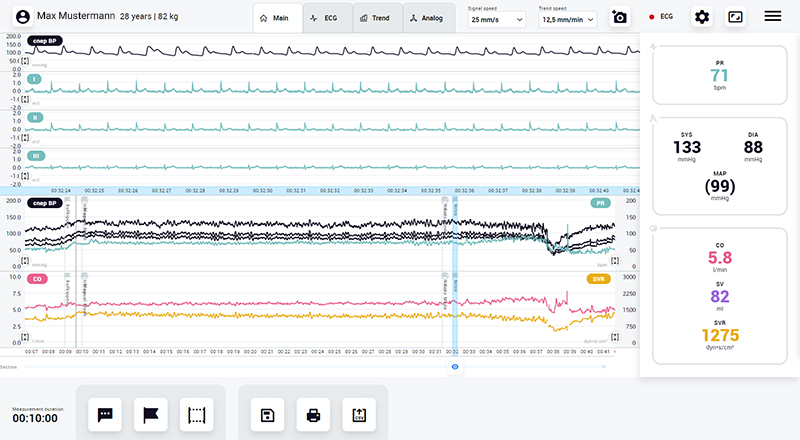
TASK FORCE® TOUCH CARDIO
ALL YOU NEED TO SUPPORT YOUR CARDIOVASCULAR ASSESSMENT




- 24″ Touchscreen
- Combination of CNAP® BP and NBP
- Advanced hemodynamics using CNAP® HD technology
- Optional 12-channel ECG
- Accessory storage
- 12-channel ECG
- Pulse Rate
- Heart Rate
- Continuous Blood Pressure
- Cardiac Output
- Systemic Vascular Resistance
- Analog Input/Output signals
- Easy & quick setup through unique finger sensor design
- New Forearm Controller with integrated sizing tool
- New Forearm Strap for safe & error-free fixation
- Disinfectable finger sensor material
- All parameters (BP, CO, SV, SVR..) from one sensor – no ICG electrodes required
- Wireless Bluetooth communication
- Electrode Contact Check
- State-of-the-art interface for smart user interaction with “touch” operation
- Integrated screenshot tool
- Set markers & comments at any time
- Easy reporting & data export
- Analog input/output interface
- Post Processing tool easy data review & documentation (paperless)
- Wireless printer support
- Wireless connection to your network drive
SYNCOPE & TILT TESTING - USEFUL LINKS
There are fantastic platforms available treating the syncope topic. Find details on efficient diagnosis and treatment.
DON´T MISS THIS EVENT!
STARS lectures and workshops on Syncope in the course of the Heart Rhythm Congress (HRC) in Birmingham – UK:

Hall 11b
Hall 3
Programme:
References:
[1] Brignole, M. et al. 2018 ESC Guidelines for the diagnosis and management of syncope. European Heart Journal vol. 39 1883–1948 (2018).
[2] Sutton, R., Ricci, F. & Fedorowski, A. Risk stratification of syncope: Current syncope guidelines and beyond. Auton. Neurosci. 238, 102929 (2021).
[3] Heartrhythmalliance: STARS. Take fainting to heart. WebPage (2022) https://www.heartrhythmalliance.org/stars/uk/take-fainting-to-heart
[4] Sheldon, R. S. et al. 2015 Heart Rhythm Society Expert Consensus Statement on the Diagnosis and Treatment of Postural Tachycardia Syndrome, Inappropriate Sinus Tachycardia, and Vasovagal Syncope HHS Public Access. Hear. Rhythm 12, 41–63 (2015).
[5] Peeters, S. Y. G., Hoek, A. E., Mollink, S. M. & Huff, J. S. Syncope: risk stratification and clinical decision making. Emerg. Med. Pract. 16, 1–22; quiz 22–3 (2014).
[6] Goldberger, Z. D. et al. ACC/AHA/HRS Versus ESC Guidelines for the Diagnosis and Management of Syncope: JACC Guideline Comparison. J. Am. Coll. Cardiol. 74, 2410–2423 (2019).
[7] Barón-Esquivias, G. et al. Head-up tilt test diagnostic yield in syncope diagnosis. J. Electrocardiol. 63, 46–50 (2020).
[8] Dan, G. A. et al. Contemporary management of patients with syncope in clinical practice: an EHRA physician-based survey. Europace 22, 980–987 (2020).
[9] Thijs, R. D. et al. Recommendations for tilt table testing and other provocative cardiovascular autonomic tests in conditions that may cause transient loss of consciousness. Auton. Neurosci. (2021) doi:10.1016/j.autneu.2021.102792.